Fenofibrate (nanoparticles).
One film-coated tablet contains 145.0mg fenofibrate (nanoparticles).
Excipients with known effect: each tablet contains: 132.00 mg of Lactose monohydrate; 145.00mg of Sucrose; 0.50mg of Soybean Lecithin.
Excipients/Inactive Ingredients: Core: Sucrose, Lactose monohydrate, silicified microcrystalline cellulose, crospovidone, Hypromellose, Sodium lauril sulfate, Docusate sodium, Magnesium stearate.
Coating: Polyvinyl alcohol, Titanium dioxide (E171), Talc, Soybean lecithin, Xanthan gum.
Serum Lipid Reducing Agents/Cholesterol and Triglycerides Reducers/Fibrates. ATC code: C10 AB 05.
Pharmacology: Pharmacodynamics: Fenofibrate is a fibric acid derivative whose lipid modifying effects reported in humans are mediated via activation of Peroxisome Proliferator Activated Receptor type alpha (PPAR∝). Through activation of PPAR∝, fenofibrate increases the lipolysis and elimination of atherogenic triglyceride-rich particles from plasma by activating lipoprotein lipase and reducing production of apoprotein C-III. Activation of PPAR∝ also induces an increase in the synthesis of apoproteins AI and AII.
The previously stated effects of fenofibrate on lipoproteins lead to a reduction in very low-and low density fractions (VLDL and LDL) containing apoprotein B and an increase in the high density lipoprotein fraction (HDL) containing apoprotein AI and AII.
In addition, through modulation of the synthesis and the catabolism of VLDL fractions fenofibrate increases the LDL clearance and reduces small dense LDL, the levels of which are elevated in the atherogenic lipoprotein phenotype, a common disorder in patients at risk for coronary heart disease.
During clinical trials with fenofibrate, total cholesterol was reduced by 20 to 25%, triglycerides by 40 to 55% and HDL cholesterol was increased by 10 to 30%.
In hypercholesterolaemic patients, where LDL cholesterol levels are reduced by 20 to 35%, the overall effect on cholesterol results in a decrease in the ratios of total cholesterol to HDL cholesterol, LDL cholesterol to HDL cholesterol, or Apo B to Apo AI, all of which are markers of atherogenic risk.
There is evidence that treatment with fibrates may reduce coronary heart disease events but they have not been shown to decrease all-cause mortality in the primary or secondary prevention of cardiovascular disease.
The Action to Control Cardiovascular Risk in Diabetes (ACCORD) lipid trial was a randomized placebo-controlled study of 5518 patients with type 2 diabetes mellitus treated with fenofibrate in addition to simvastatin. Fenofibrate plus simvastatin therapy did not show any significant differences compared to simvastatin monotherapy in the composite primary outcome of non-fatal myocardial infarction, non-fatal stroke, and cardiovascular death (hazard ratio [HR] 0.92, 95% CI 0.79-1.08, p = 0.32; absolute risk reduction: 0.74%). In the pre-specified subgroup of dyslipidaemic patients, defined as those in the lowest tertile of HDL-C (≤34 mg/dl or 0.88 mmol/L) and highest tertile of TG (≥204 mg/dl or 2.3 mmol/L) at baseline, fenofibrate plus simvastatin therapy demonstrated a 31% relative reduction compared to simvastatin monotherapy for the composite primary outcome (hazard ratio [HR] 0.69, 95% CI 0.49-0.97, p = 0.03; absolute risk reduction: 4.95%). Another prespecified subgroup analysis identified a statistically significant treatment-by-gender interaction (p = 0.01) indicating a possible treatment benefit of combination therapy in men (p=0.037) but a potentially higher risk for the primary outcome in women treated with combination therapy compared to simvastatin monotherapy (p=0.069). This was not observed in the aforementioned subgroup of patients with dyslipidaemia but there was also no clear evidence of benefit in dyslipidaemic women treated with fenofibrate plus simvastatin, and a possible harmful effect in this subgroup could not be excluded.
Extravascular deposits of cholesterol (tendinous and tuberous xanthoma) may be markedly reduced or even entirely eliminated during fenofibrate therapy.
Patients with raised levels of fibrinogen treated with fenofibrate have shown significant reductions in this parameter, as have those with raised levels of Lp(a). Other inflammatory markers such as C Reactive Protein are reduced with fenofibrate treatment.
The uricosuric effect of fenofibrate leading to reduction in uric acid levels of approximately 25% should be of additional benefit in those dyslipidaemic patients with hyperuricaemia.
Fenofibrate has been shown to possess an anti-aggregatory effect on platelets in animals and in a clinical study, which showed a reduction in platelet aggregation induced by ADP, arachidonic acid and epinephrine.
Effects of fenofibrate on the reduction of the progression of microvascular complications in patients with type 2 of diabetes mellitus have been proven in international randomized placebo-controlled trials.
In the ACCORD trial (in a subgroup of 1953 patients, ACCORD-eye substudy) the progression of diabetic retinopathy by 3 or more steps on the Early Treatment Diabetic Retinopathy Study (ETDRS) Severity Scale was 6.5% with fenofibrate and simvastatin combined with dyslipidemia therapy, versus 10.2% with simvastatin and placebo therapy (adjusted odds ratio, 0.60; 95% CI, 0.42 to 0.87; P=0.006).
Fenofibrate therapy was also associated with lower frequency of laser treatment required for retinopathy (5.2% vs 3.6%, p=0.0003) in the FIELD study.
Pharmacokinetics: LIPANTHYL PENTA 145 mg, film-coated tablets contains 145 mg of fenofibrate nanoparticles.
Absorption: Maximum plasma concentrations (Cmax) occur within 2 to 4 hours after oral administration. Plasma concentrations are stable during continuous treatment in any given individual.
Contrarily to previous fenofibrate formulations, the maximum plasma concentration and overall exposure of the nanoparticle formulation is independent from food intake. Therefore, LIPANTHYL PENTA 145, film-coated tablet may be taken without regard to meals.
A food-effect study involving administration of the new 145 mg tablet formulation of fenofibrate to healthy male and female subjects under fasting conditions and with a high fat meal indicated that exposure (AUC and Cmax) to fenofibric acid is not affected by food.
Distribution: Fenofibric acid is strongly bound to plasma albumin (more than 99%).
Metabolism and excretion: After oral administration, fenofibrate is rapidly hydrolysed by esterases to the active metabolite fenofibric acid. No unchanged fenofibrate can be detected in the plasma. Fenofibrate is not a substrate for CYP 3A4. No hepatic microsomal metabolism is involved.
The drug is excreted mainly in the urine. Practically all the drug is eliminated within 6 days. Fenofibrate is mainly excreted in the form of fenofibric acid and its glucuronide conjugate. In elderly patients, the fenofibric acid apparent total plasma clearance is not modified.
Kinetic studies following the administration of a single dose and continuous treatment have demonstrated that the drug does not accumulate. Fenofibric acid is not eliminated by haemodialysis.
The plasma elimination half-life of fenofibric acid is approximately 20 hours.
Toxicology: Preclinical safety data: Acute toxicity studies have yielded no relevant information about specific toxicity of fenofibrate.
In a three-month oral nonclinical study in the rat species with fenofibric acid, the active metabolite of fenofibrate, toxicity for the skeletal muscles (particularly those rich in type I - slow oxidative - myofibres) and cardiac degeneration, anemia and decreased body weight were seen at exposure levels ≥50-fold the human exposure for the skeletal toxicity and >15 fold for the cardiomyotoxicity.
Reversible ulcers and erosions in the gastro-intestinal tract occurred in dogs treated during 3 months at exposures approximately 7-fold the clinical AUC.
Studies on mutagenicity of fenofibrate have been negative.
In rats and mice, liver tumours have been found at high dosages, which are attributable to peroxisome proliferation. These changes are specific to small rodents and have not been observed in other animal species. This is of no relevance to therapeutic use in man.
Studies in mice, rats and rabbits did not reveal any teratogenic effect. Embryotoxic effects were observed at doses in the range of maternal toxicity. Prolongation of the gestation period and difficulties during delivery were observed at high doses.
No effects on fertility were detected in non-clinical reproductive toxicity studies conducted with fenofibrate. However reversible hypospermia and testicular vacuolation and immaturity of the ovaries were observed in a repeat-dose toxicity study with fenofibric acid in young dogs.
LIPANTHYL PENTA 145, film-coated tablet is indicated as an adjunct to diet and other non-pharmacological treatment (e.g. exercise, weight reduction) for the following: Treatment of severe hypertriglyceridaemia with or without low HDL cholesterol.
Mixed hyperlipidaemia when a statin is contraindicated or not tolerated.
Mixed hyperlipidaemia in patients at high cardiovascular risk in addition to a statin when triglycerides and HDL cholesterol are not adequately controlled.
LIPANTHYL PENTA 145, film-coated tablet is indicated for the reduction in the progression of diabetic retinopathy in patients with type 2 diabetes and existing diabetic retinopathy. Lipanthyl does not replace the appropriate control of blood pressure, blood glucose and blood lipids in reducing the progression of diabetic.
Response to therapy should be monitored by determination of serum lipid values. If an adequate response has not been achieved after several months (e.g. 3 months), complementary or different therapeutic measures should be considered.
Posology: Adults: The recommended dose is one tablet containing 145mg fenofibrate taken once daily. Patients currently taking one 200 mg capsule (or one 160 mg tablet) can be changed to one 145mg fenofibrate tablet without further dose adjustment.
Special Populations: Geriatric Populations: In elderly patients, without renal impairment, the usual adult dose is recommended.
Dosage reduction is required in patients with renal impairment. In moderate chronic kidney disease (creatinine clearance 30 to 60mL/min), and if a low dose is available, start with one capsule of 100mg standard once daily.
If no low dose is available, then fenofibrate is not recommended.
In patients with severe chronic kidney disease (creatinine clearance < 30ml/min), fenofibrate is contraindicated.
Hepatic impairment: Fenofibrate 145mg tablet is not recommended for use in patients with hepatic impairment due to the lack of data.
Pediatric population: The safety and efficacy of fenofibrate in children and adolescents younger than 18 years has not been established. No data are available. Therefore the use of fenofibrate is not recommended in paediatric subjects under 18 years.
Method of administration: LIPANTHYL PENTA 145, film-coated tablet may be given at any time of the day, with or without food (see Pharmacology: Pharmacokinetics under Actions). Tablet should be swallowed whole with a glass of water.
Only anecdotal cases of fenofibrate overdosage have been received. In the majority of cases no overdose symptoms were reported.
No specific antidote is known. If an overdose is suspected, treat symptomatically and institute appropriate supportive measures as required. Fenofibrate cannot be eliminated by haemodialysis.
Hepatic in sufficiency (including biliary cirrhosis and unexplained persistent liver function abnormality).
Known gallbladder disease.
Severe chronic kidney disease.
Chronic or acute pancreatitis with the exception of acute pancreatitis due to severe hypertriglyceridemia.
Known photoallergy or phototoxic reaction during treatment with fibrates or ketoprofen.
Hypersensitivity to fenofibrate or to any of the excipients listed in Description.
LIPANTHYL PENTA 145, film-coated tablet should not be taken in patients allergic to peanut or arachis oil or soybean lecithin or related products due to the risk of hypersensitivity reactions.
Secondary causes of hyperlipidemia: Secondary cause of hyperlipidemia, such as uncontrolled type 2 diabetes mellitus, hypothyroidism, nephrotic syndrome, dysproteinemia, obstructive liver disease, pharmacological treatment, alcoholism, should be adequately treated before fenofibrate therapy is considered. For hyperlipidaemic patients taking estrogens or contraceptives containing oestrogens it should be ascertained whether the hyperlipidaemia is of primary or secondary nature (possible elevation of lipid values caused by oral oestrogen).
Liver function: As with other lipid lowering agents, increases have been reported in transaminase levels in some patients. In the majority of cases these elevations were transient, minor and a symptomatic. It is recommended that transaminase levels be monitored every 3 months during the first 12 months of treatment. Attention should be paid to patients who develop increase in transaminase levels and therapy should be discontinued if ASAT (SGOT) and ALAT (SGPT) levels increase to more than 3 times the upper limit of the normal range. When symptoms indicative of hepatitis occur (e.g. jaundice, pruritus), and diagnosis is confirmed by laboratory testing, fenofibrate therapy should be discontinued.
Pancreas: Pancreatitis have been reported in patients taking fenofibrate (see Contraindications and Adverse Reactions). This occurrence may represent a failure of efficacy in patients with severe hypertriglyceridemia, a direct drug effect, or a secondary phenomenon mediated through biliary tract stone or sludge formation with obstruction of the common bile duct.
Muscle: Muscle toxicity, including very rare cases of rhabdomyolysis, with or without renal failure, has been reported with administration of fibrates and other lipid-lowering agents. The incidence of this disorder increases in case of hypoalbuminemia and previous renal insufficiency. Patients with pre-disposing factors for myopathy and/or rhabdomyolysis, including age above 70 years old, personal or familial history of hereditary muscular disorders, renal impairment, hypothyroidism and high alcohol intake, may be at an increased risk of developing rhabdomyolysis. For these patients, the putative benefits and risks of fenofibrate therapy should be care fully weighed up.
Muscle toxicity should be suspected in patients presenting diffuse myalgia, myositis, muscular cramps and weakness and/or marked increases in CPK (levels exceeding 5 times the upper normal range). In such cases treatment with fenofibrate should be stopped.
The risk of muscle toxicity may be increased if the drug is administered with another fibrate or an HMG CoA reductase inhibitor, especially in cases of pre-existing muscular disease. Consequently, the co-prescription of fenofibrate with HMG CoA reductase inhibitor or another fibrate should be reserved to patients with severe combined dyslipidaemia and high cardiovascular risk without any history of muscular disease and with a close monitoring of potential muscle toxicity.
Renal function: Treatment should be interrupted in case of an increase in creatinine levels >50% of (upper limit of normal). It is recommended that creatinine is measured during the first three months after initiation of treatment and thereafter periodically (for dose recommendations, see Dosage & Administration).
Excipients: As this medicinal product contains lactose patients with rare hereditary problems of galactose intolerance, Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
As this medicinal product contains sucrose, patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase in sufficiency should not take this medicine.
Effects on the ability to drive and use machines: LIPANTHYL PENTA145, film-coated tablet has no or negligible influence on the ability to drive and use machines.
Fertility: Reversible effects on fertility have been observed in animals (see Pharmacology: Toxicology: Preclinical safety data under Actions). There are no clinical data on fertility from the use of Lipanthyl Penta 145mg.
Pregnancy: There are no adequate data from the use of fenofibrate in pregnant women. Animal studies have not demonstrated any teratogenic effects. Embryotoxic effects have been shown at doses in the range of maternal toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions). The potential risk for humans is unknown. Therefore, fenofibrate should only be used during pregnancy after a careful benefit/risk assessment.
Lactation: It is unknown whether fenofibrate and/or its metabolites are excreted in human milk. A risk to the suckling child cannot be excluded. Therefore fenofibrate should not be used during breast-feeding (see Contraindications).
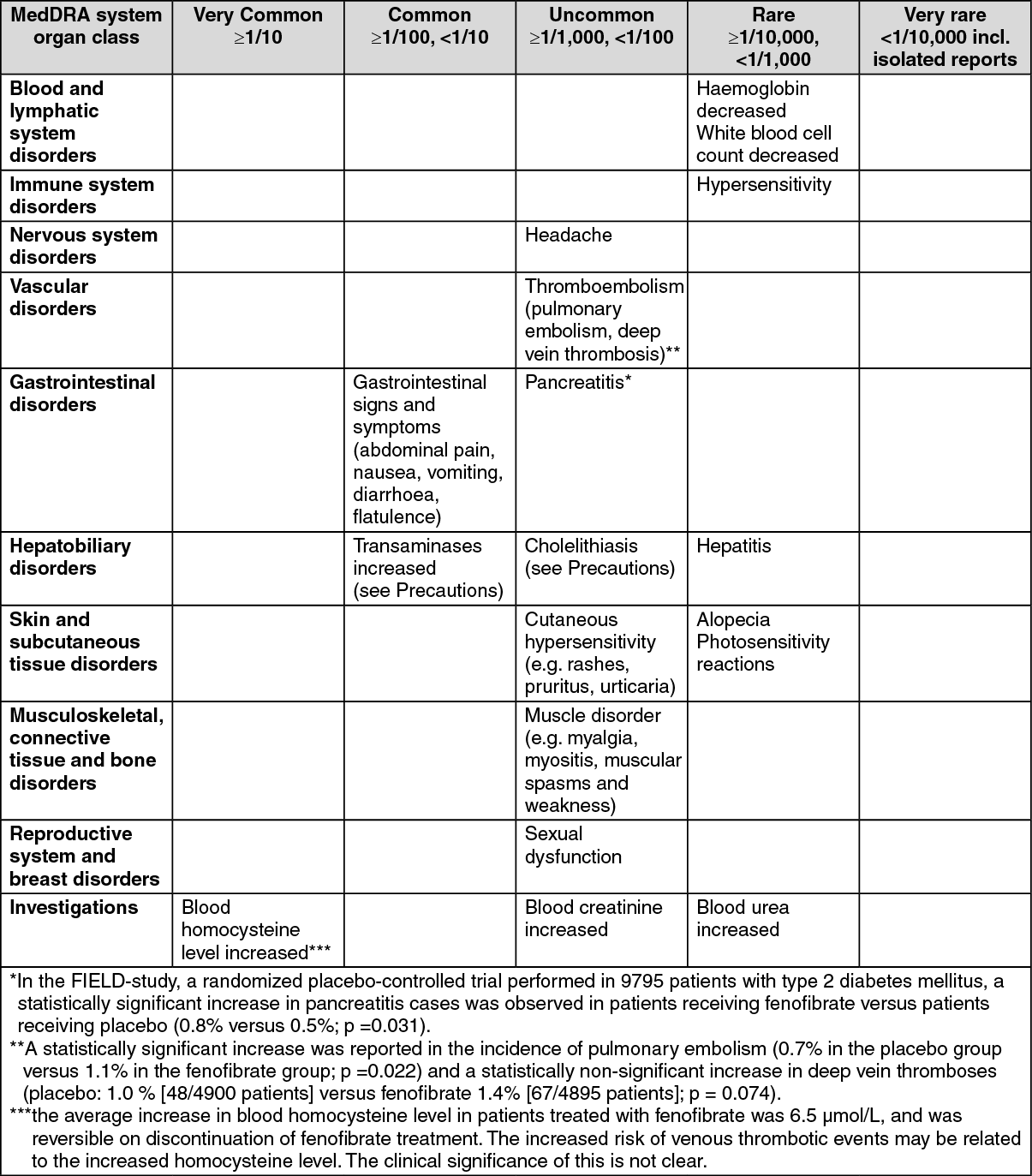
The most commonly reported ADRs during LIPANTHYL PENTA 145, film-coated therapy are digestive, gastric or intestinal disorders.
The following undesirable effects have been observed during placebo-controlled clinical trials (n=2344) with the below indicated frequencies: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In addition to those events reported during clinical trials, the following side effects have been reported spontaneously during post-marketing use of LIPANTHYL PENTA 145, film-coated. A precise frequency cannot be estimated from the available data and is therefore classified as "not known":
Respiratory, thoracic and mediastinal disorders: Interstitial lung disease.
Musculoskeletal, connective tissue and bone disorders: Rhabdomyolysis.
Hepatobiliary disorders: jaundice, complications of cholelithiasis (e.g. cholecystitis, cholangitis, biliary colic).
Skin and Subcutaneous Tissue Disorders: severe cutaneous reactions (e.g erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis).
Nervous system disorders: Fatigue.
Oral anticoagulants: Fenofibrate enhances oral anticoagulant effect and may increase risk of bleeding. It is recommended that the dose of anticoagulants is reduced by about one third at the start of treatment and then gradually adjusted if necessary according to INR (International Normalised Ratio) monitoring.
Cyclosporin: Some severe cases of reversible renal function impairment have been reported during concomitant administration of fenofibrate and cyclosporin. The renal function of these patients must therefore be closely monitored and the treatment with fenofibrate stopped in the case of severe alteration of laboratory parameters.
HMG-CoA reductase inhibitors and other fibrates: The risk of serious muscle toxicity is increased if a fibrate is used concomitantly with HMG-CoA reductase inhibitors or other fibrates. Such combination therapy should be used with caution and patients monitored closely for signs of muscle toxicity (see Precautions).
Glitazones: Some cases of reversible paradoxical reduction of HDL-cholesterol have been reported during concomitant administration of fenofibrate and glitazones. Therefore, it is recommended to monitor HDL-cholesterol if one of these components is added to the other and stopping of either therapy if HDL-cholesterol is too low.
Cytochrome P450 enzymes: In vitro studies using human liver microsomes indicate that fenofibrate and fenofibric acid are not inhibitors of cytochrome (CYP) P450 isoforms CYP3A4, CYP2D6, CYP2E1, or CYP1A2. They are weak inhibitors of CYP2C19 and CYP2A6, and mild-to-moderate inhibitors of CYP2C9 at therapeutic concentrations.
Patients co-administered fenofibrate and CYP2C19, CYP2A6, and especially CYP2C9 metabolised drugs with a narrow therapeutic index should be carefully monitored and, if necessary, dose adjustment of these drugs is recommended.
Incompatibilities: Not applicable.
Instructions for use and handling: No special requirements.
Shelf-life: 3 years.
Store in the original package, at a temperature not exceeding 30°C.
C10AB05 - fenofibrate ; Belongs to the class of fibrates. Used in the treatment of hyperlipidemia.
Lipanthyl Penta 145 FC tab 145 mg
30's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
